Lunar Effects on Mood and Biology Are Real
 Last week in North America we saw the largest Super Moon of the year so far – it was called the “Super Snow Moon”. At the same time, I had several clients have strangely aberrant reactions to their neurofeedback sessions, as well as several friends on facebook making particularly emotional posts and complaining of feeling crazy, including myself. I thought it might be a reaction to how I felt the week before with a bunch of stressors, but then my father said something in passing about the supermoon and I wondered if there really might be a connection.
Last week in North America we saw the largest Super Moon of the year so far – it was called the “Super Snow Moon”. At the same time, I had several clients have strangely aberrant reactions to their neurofeedback sessions, as well as several friends on facebook making particularly emotional posts and complaining of feeling crazy, including myself. I thought it might be a reaction to how I felt the week before with a bunch of stressors, but then my father said something in passing about the supermoon and I wondered if there really might be a connection.
At the gym, a woman who is a former counselor who used to work at an emergency call center talked about how they would joke every full moon about how many more calls they expected to get. Others weighed in with their stories of eventful “coincidences” when you could essentially count out 9 months after a really bad storm and then there would be a bunch of babies suddenly being born around the same time (implying that couples tend to “get it on” more during storms, thus increasing the pregnancy rates at those times). Anyway, this could all just be our brains looking for connections where there may or may not be any, right? So I decided to take a look into the literature.
You see, my father has a Ph.D. physics. He actually warned me against writing this post since he worries that it’ll come across as pseudo-science and people will reject it and me and think we’re a bunch of dummies, I guess. I’m not entirely sure because I told him I write what I’m interested in and if he wants to write a post he is very welcome to do so. In any case, he is the one who mentioned the moon connection in the first place to me, so I find that interesting. He said that since the moon affects Earths magnetic field, it could also possibly affect any of us who are affected by Earth’s magnetic field. Well, we know that birds use Earth’s magnetic field to navigate, so why wouldn’t we have some connection with it? Why wouldn’t human biology also be affected by changes in earth’s magnetic field?
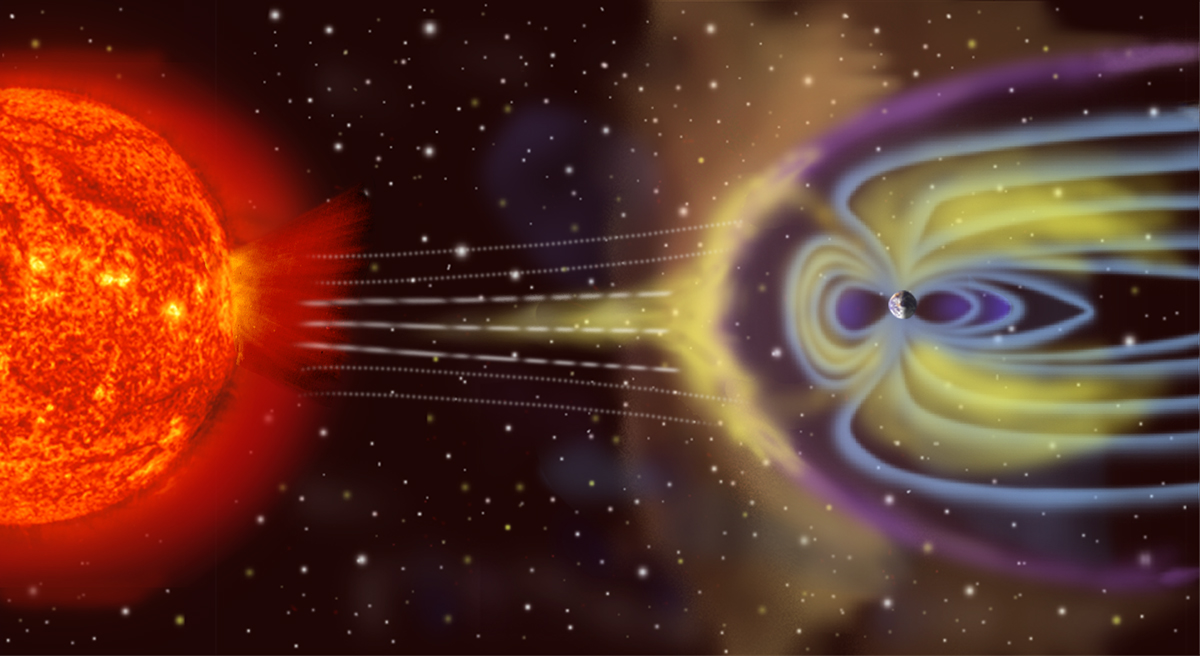
The answer is yes, human (and other animal and plant) biology is, indeed, affected by the the phases of the moon, which may be explained by sensing changes in the “magnetosphere” (the magnetic field surrounding the earth), but not so much by the gravitational or light effe cts by the moon. In a paper titled, “Lunar biological effects and the magnetosphere“, Michael Bevington describes the evidence for lunar biological effects and how they are most-likely explained by the full moon traversing the moon’s “magnetotail”, an electromagnetic plasma sheet that extends out from the surface of the Earth opposite the sun (and its spiraling solar wind). When the moon crosses the magnetotail’s sheet, it attracts a large electrical charge, increasing the electric field on the dark side of the moon, which causes ions from the moon’s surface to transfer to the Earth’s magnetosphere and increase the Earth’s electromagnetic field, creating a magnetosphere feedback mechanism.
cts by the moon. In a paper titled, “Lunar biological effects and the magnetosphere“, Michael Bevington describes the evidence for lunar biological effects and how they are most-likely explained by the full moon traversing the moon’s “magnetotail”, an electromagnetic plasma sheet that extends out from the surface of the Earth opposite the sun (and its spiraling solar wind). When the moon crosses the magnetotail’s sheet, it attracts a large electrical charge, increasing the electric field on the dark side of the moon, which causes ions from the moon’s surface to transfer to the Earth’s magnetosphere and increase the Earth’s electromagnetic field, creating a magnetosphere feedback mechanism.
Here are some of the reported effects of the full moon on animal and plant biology (summarized in the above-mentioned article): tree diameter variation reflects a lunar rhythm; reproduction, changes in the stress hormone, glucocorticoid, and foraging by mice follow a lunar rhythm; epileptic seizures increase by over 1.5 times during a full moon, as well as the number of sudden unexpected deaths in epilepsy (highest [70%] during the full moon); the number of patients with violent and acute behavioral disturbances doubled during the full moon compared to other lunar phases; and a recent study showed that bipolar mood cycles correlated with lunar phases in 17 patients with rapid cycling bipolar affective disorder. Then, of course, there are many more anecdotal reports from doctors at hospitals and others who say that they see an increase in patients coming in during the full moon, etc.
The prevailing belief that the full moon affects human biology has been around for millennia, and many authors tend to cite the ancient Roman philosopher and naval and army commander, Pliny the Elder, as the first to make the connection between the lunar phases and the tides. He also was able to see the correlation with shellfish and other sea creature growth and suggested that the moon had nourishing powers. It used to be a given that humans believed in the biological effects of the full moon, but in the last century or so, scientists have had a hard time gathering enough evidence to demonstrate a causal effect, which is understandable seeing as all you really can do is maybe show a correlation due to not being able to isolate or control all the confounding factors involved. Even the correlative effects are not 100% penetrant (meaning, not everyone is affected by the full moon or other lunar phases). Having a scientific explanation and mechanism for how the lunar phases (particularly the full moon) affects biology is also important for determining the likelihood of biological effects. Unfortunately, most attempts at finding an explanation have fallen short, such as mechanisms involving the gravitational effects of the moon or the light effects of a full moon. I will not go into detail about why those fail, but I refer the reader to the initial article that I linked to this blog for such detailed information.
Suffice it to say, the best explanatory mechanism for how the full moon affects biology is its effects on Earth’s electromagnetic field. As described above, as the full moon traverses the magnetotail of the magnetosphere, it causes a feedback mechanism between the Earth and the Moon to increase the potential of the electric field on Earth by 1-7 V/m (measured by Michael Bevington). 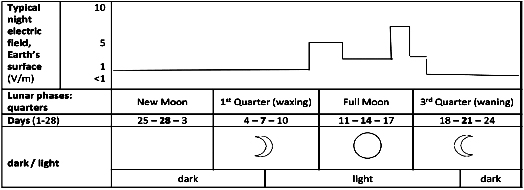 In fact, the measurements show that the greatest change in the potential occurs as the moon crosses into and out of the magnetotail plasma, which occurs 2-3 days before the full moon and 3-4 days after the full moon (Table 1 below and depicted in the figure on the right).
In fact, the measurements show that the greatest change in the potential occurs as the moon crosses into and out of the magnetotail plasma, which occurs 2-3 days before the full moon and 3-4 days after the full moon (Table 1 below and depicted in the figure on the right).
It is true that 1-7 V/m is a very weak electromagnetic field, but if you consider that the electrical potentials of the cerebral cortex, as measured from the scalp by electroencephalography (EEG), are generally in the micro-volt to milli-volt range (meaning 0.001 – 0.000001 V range), and that neurons are generally holding an electrical potential difference across its membrane around 70 mV (0.07 V), this suggests that 1-7 volts could have pretty dramatic effects on the human body. However, until very recently, scientists did not believe that the human body could perceive changes in electric fields (EFs) at such small levels. It was previously thought that humans can only detect static EFs (like that at the surface of the Earth) through its changes in electrical discharges on the surface of the body and their interaction with body hair or the creation of micro-shocks, but a recent meta-analysis concluded that “5% of the participants could detect a static EF below 20 kV/m, 33% of the subjects detected a static EF below 40 kV/m and 66% detected fields below 50 kV/m“. Of course, these EFs are much, much greater than that which were measured at the surface of the Earth by Michael Bevington at 1-7 V/m around the time of a full moon, so we still cannot claim that a large proportion of people can likely detect the 1-7 V/m change in the Earth’s EF during a full moon.
But last week’s full moon wasn’t any old full moon, it was a SUPER MOON, 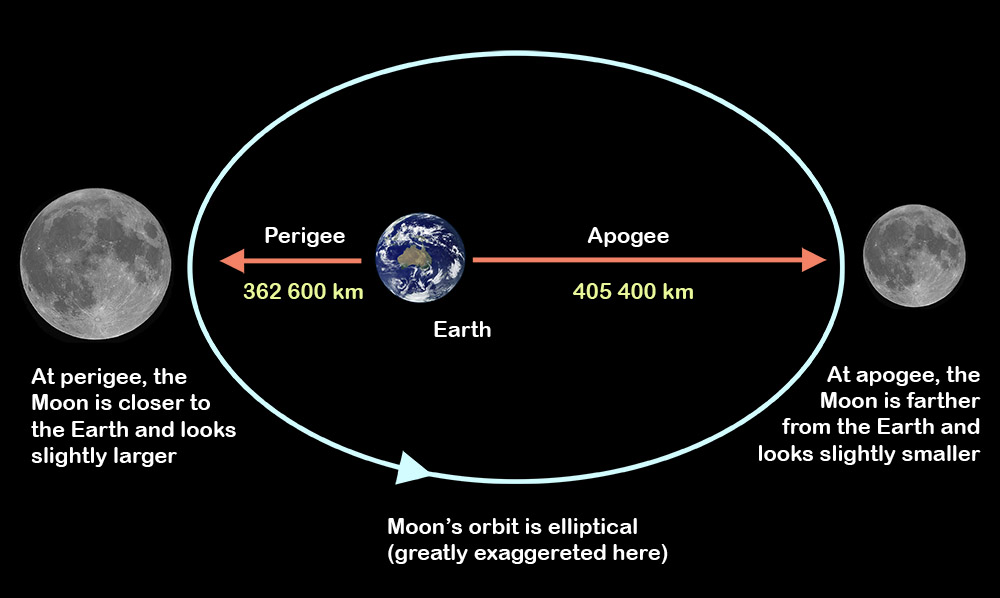 which is a special kind of full moon when the moon is at its closest point (perigee) to the Earth on its elliptical orbit around the Earth. Not only does this make the moon appear larger, but it also means that it passes through more of the magnetotail than a regular full moon, and it also increases the feedback mechanism and electromagnetic strength between the Earth and the moon. Therefore, we can hypothesize that the increase in electrical potential at the surface of the Earth would be much greater during a super full moon than during a regular full moon, although I don’t know how much greater that might be, but I’m sure someone with better math and physics skills than me could make a decent estimation (like my father!). Furthermore, the intensity of the EF at the surface of the Earth increases with moisture like rain or snow, which we certainly have in abundancy in the Pacific Northwest! So, altogether, it seems that we had two additional factors that increased the intensity of the effects of the full moon on us in the Pacific Northwest last week – a super moon and lots of rain and snow.
which is a special kind of full moon when the moon is at its closest point (perigee) to the Earth on its elliptical orbit around the Earth. Not only does this make the moon appear larger, but it also means that it passes through more of the magnetotail than a regular full moon, and it also increases the feedback mechanism and electromagnetic strength between the Earth and the moon. Therefore, we can hypothesize that the increase in electrical potential at the surface of the Earth would be much greater during a super full moon than during a regular full moon, although I don’t know how much greater that might be, but I’m sure someone with better math and physics skills than me could make a decent estimation (like my father!). Furthermore, the intensity of the EF at the surface of the Earth increases with moisture like rain or snow, which we certainly have in abundancy in the Pacific Northwest! So, altogether, it seems that we had two additional factors that increased the intensity of the effects of the full moon on us in the Pacific Northwest last week – a super moon and lots of rain and snow.
There are a few more pieces of this puzzle that I want to add but are hard to place in this post. One is that Michael Bevington’s measurements of the electric field potentials at the surface of the Earth are a little misleading, since the truth is that there is a gradient in the electrical potential from the surface of the Earth to the outer atmosphere and beyond. This gradient is typically between 0.3 – 120 V/m, while it is typically less than 1 V/m under 30 km from the Earth (in concurrence with Michael Bevington’s measurements). I just wanted to mention this because it does matter where you measure the EF potential (and it changes throughout the day/night, whether over land or water, etc.). I would like to measure the EF at the surface of the Earth during a regular full moon and also during a Super full moon to test my hypothesis that the super full moon increases the EF potential even more than a regular full moon (ideally I’d also measure the “apogee” full moon, aka “micromoon”, because that should change the potential even less).
A recent report suggests that humans might actually have a type of 6th sense in which we can perceive magnetic fields (particularly, the Earth’s magnetic field). Of course, this is not the same as detecting a static electric field, but geophysicist Joe Kirschvink at Caltech was able to demonstrate that a weak magenetic field could change the brainwaves of two dozen subjects in a Faraday cage (to block out ambient electromagnetic noise). Specifically, he observed a decrease in alpha waves (it makes sense that he looked at alpha waves since alpha is the easiest brainwave to detect in typical/”normal” humans). Since alpha brainwaves are considered “standby mode” brainwaves that increase synchronously when the brain is not processing information in that region, Kirschvink’s results indicate that these brains were being activated (or agitated) when sensing the changing magnetic fields, or it could merely mean that the brains were processing the perceptual information of the changing magnetic fields (thus, no longer in “standby mode”).
Lastly, I want to acknowledge the fact that there are people who are highly sensitive to or who have highly unusual interactions with electromagnetic fields. I’m referring to people who have many adverse reactions when using their cell phone, computer, or when working under fluorescent lights, etc., as well as people who may walk in a room and cause the lights to flicker or who may be constantly causing their electrical devices to blow fuses, etc. There are probably more of the former than the latter, but the existence of both is considered controversial in the scientific community, although there have been many studies trying to ascertain whether or not Electromagnetic (Hyper)Sensitivity exists as a real syndrome. I personally do not need a huge epidemiological study to know that there are some people who are highly sensitive to electromagnetic field (EMF) changes, but I can understand the need for such studies in order to determine what measures we may need to take to regulate the amount of electromagnetic radiation we are exposed to for public health’s sake. Otherwise, it’s a matter of individual choices, so why argue with someone if they say they are highly sensitive to electromagnetic radiation? If it doesn’t affect you, why do you need to judge whether or not their symptoms are really caused by the electromagnetic radiation? Plus, maybe the studies showing no correlation aren’t probing the problem appropriately. Such as, maybe there are more pieces of the puzzle missing when they try to do experiments in a lab where they alter the EF potential and ask the subjects if they can sense a difference or if they are having any adverse effects. The EF may be one of several factors that either add up and/or synergize to cause the adverse effects. In any case, I think, as a society, we are too quick to judge each other on our individual differences, especially when it comes to perception. One person can never truly know how another person perceives something, and that is just the way it is. It’s the natural limitation of being separate beings. We can, however, make predictions and test hypotheses to determine if pieces of our model of how differences in perception work, which, if confirmed, can only bolster the validity of our perceptions. This is, of course, the scientific approach to a subjective experience, which can never truly be understood scientifically.





Recent Comments